

The Person Before the Institution
Why Institutional Ethics Has to Begin With the Person

A patient can be in the chart and still not be seen.
A student can be in the file and still not be known.
A disabled person can fit the category and still be reduced by it.
Modern institutions do not fail people simply by ignoring them. Often, they see people under descriptions that replace them. The person becomes the diagnosis. The student becomes the score. The applicant becomes the case. The incarcerated person becomes the risk profile.
That is why a theory of institutional life has to begin with a theory of the person.
Institutions classify, document, diagnose, score, evaluate, educate, punish, treat, authorize, deny, and repair. None of these acts creates the person.
The person arrives before the institution does.
Personhood is not an achievement of documentation, eligibility, legal status, diagnosis, or procedural inclusion. A person does not become worthy because a system has learned how to process them.
They are already worthy.
That is the foundation.
This means the person must never be treated merely as an object of use, management, calculation, or administrative convenience.
Institutions need categories to act. A diagnosis guides treatment. A disability category secures accommodation. A risk designation may prevent harm. A file preserves memory across time and distance.
These forms can be necessary. They can even be protective.
But they become ethically dangerous the moment they stop serving the person and start standing in the person’s place.
The question is never whether institutions may classify persons. They must.
The ethical problem is not mediation itself. Institutions must mediate their response through forms. The danger begins when mediation becomes replacement.
The question is whether classification remains morally subordinate to the person being classified.
Irreducible personhood
I call this foundation irreducible personhood.
A person always exceeds any category, diagnosis, score, file, risk level, eligibility status, or institutional description through which they become known.
This does not mean such descriptions are always false. A diagnosis may be clinically accurate. A score may be predictive. A record may preserve important facts.
But even when descriptions are accurate, they do not exhaust the moral reality of the person.
A patient is more than a diagnosis.
A student is more than a file.
An incarcerated person is more than a risk score.
A disabled person is more than an eligibility category.
A poor person is more than a benefits status.
The institutional form makes something visible. It does not make the person fully known.
The danger of substitution
The specific danger here is substitution.
Reduction narrows the person.
Substitution replaces the person.
Reduction treats one part of a person as though it were the whole. Substitution goes further: the institutional representation becomes the object of response.
The institution no longer responds to the person through the category. It responds to the category as if the category were the person.
The patient becomes the diagnosis.
The student becomes the score.
The incarcerated person becomes the risk profile.
The person remains physically present but has been institutionally displaced. The form now occupies the moral place where the person should remain.
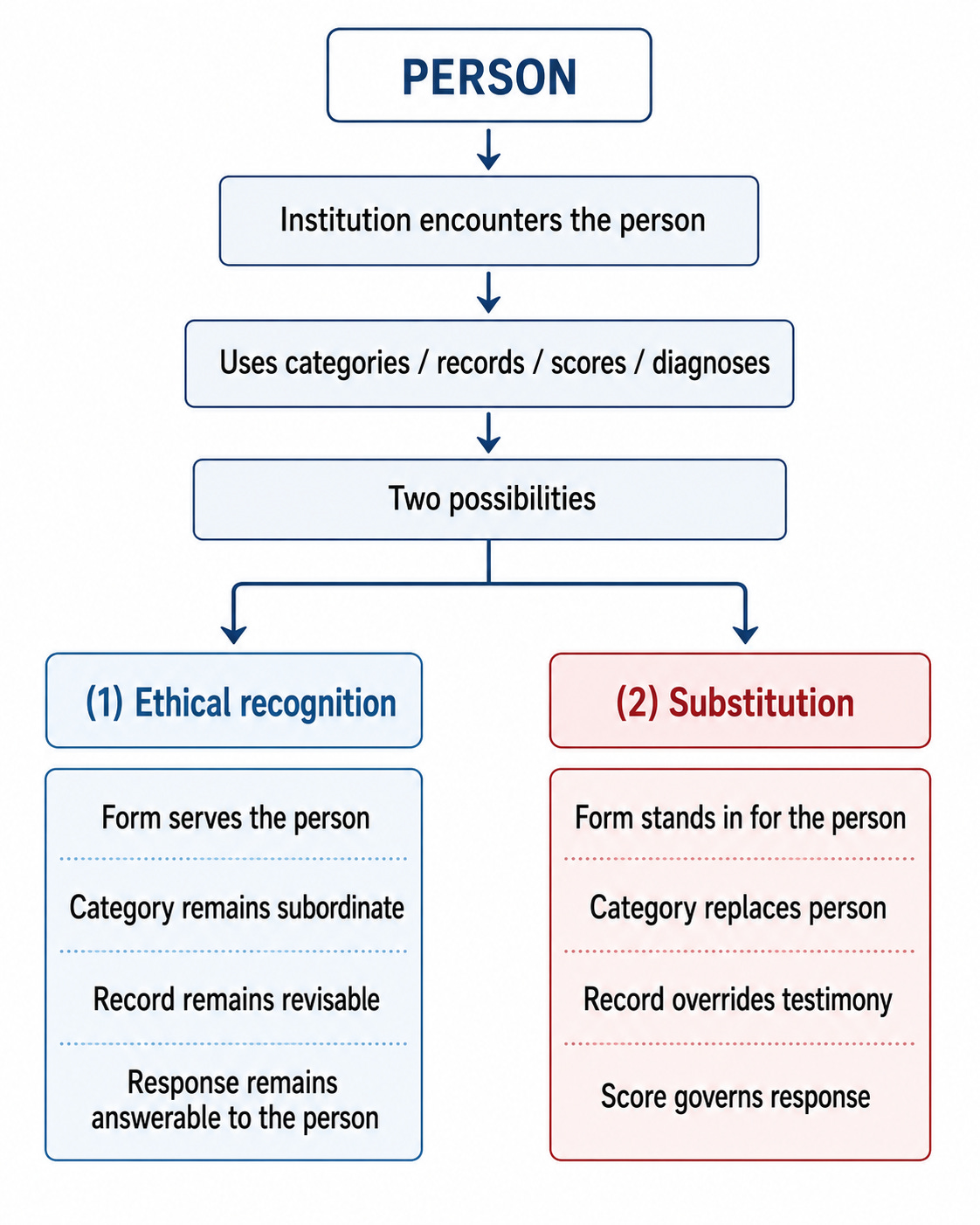
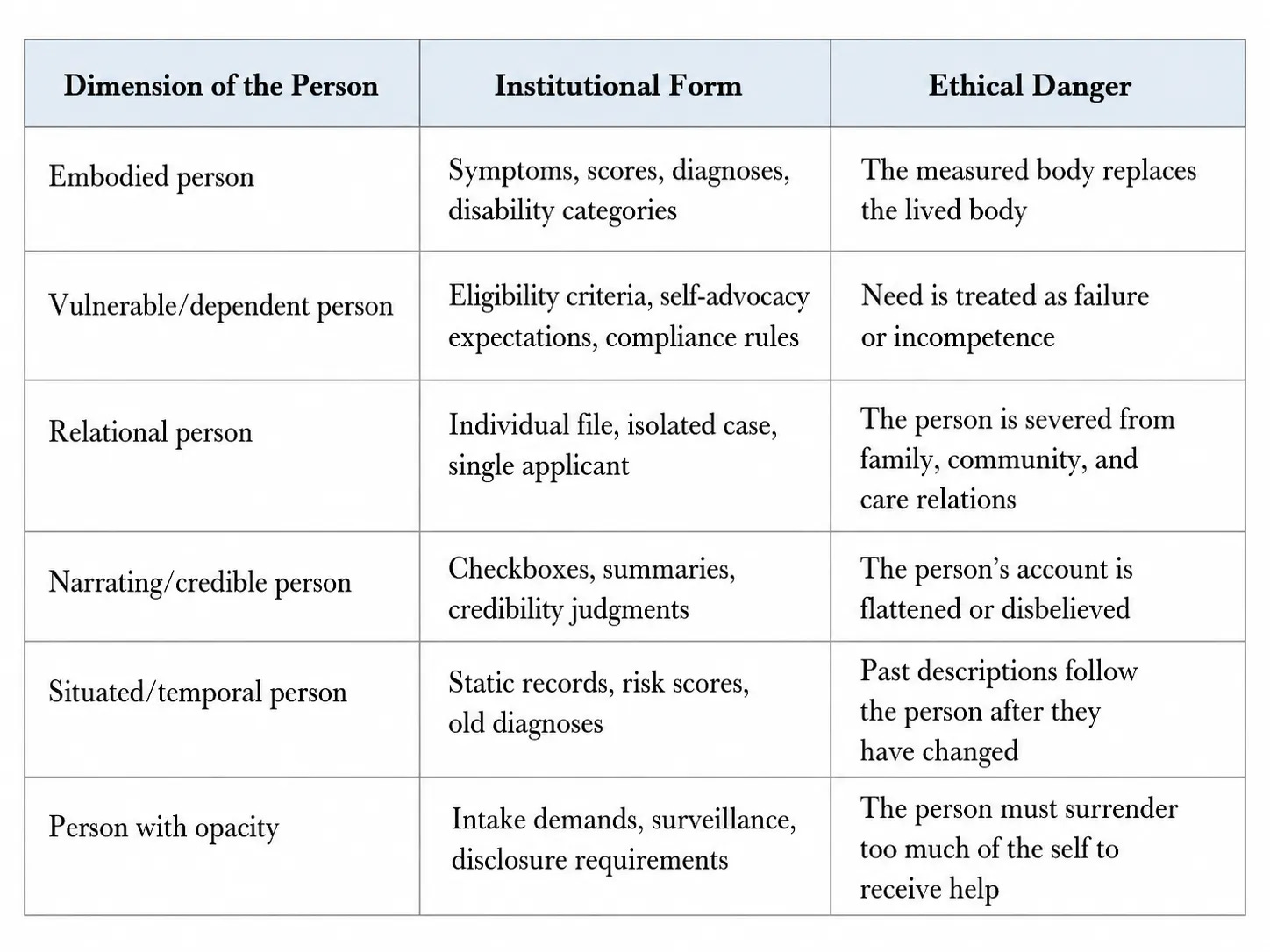
What follows is not a division of personhood into parts. It is a map of the places where institutions most often substitute the form for the person. The figure above shows the general ethical movement: institutional forms either remain answerable to the person or begin to replace the person as the object of response. The table below identifies the recurring sites where that replacement most often occurs.
The embodied person
The person is embodied.
Human beings do not approach institutions as abstract rational wills. They come through bodies that suffer, age, hunger, labor, heal, deteriorate, and depend.
Institutions typically know bodies through symptoms, measurements, diagnoses, disability categories, wounds, vital signs, and records.
These forms may be necessary. But the measured body must not replace the lived body.
Pain is more than a numeric score.
Disability is more than functional limitation.
Illness is more than a diagnostic code.
Consider a patient who rates their pain a four on a ten-point scale because they have learned that higher numbers trigger doubt rather than response. The number entered the record. The experience did not.
The embodied person exceeds the institution’s reading of the body.
The vulnerable and dependent person
The person is also vulnerable and dependent.
Dependency is not a failure of personhood. Vulnerability is not an exception to dignity. Need does not diminish moral standing. It generates a claim on response.
Institutions often encounter persons precisely when they are least able to satisfy institutional expectations: when they are sick, disabled, hungry, afraid, confused, punished, displaced, aging, or unable to speak in approved terms.
A person may be fully a person at the exact moment they cannot advocate for themselves, document their situation, explain themselves clearly, or perform the kind of credibility the system expects.
An institution that recognizes only the articulate, organized, and self-sufficient has not recognized personhood.
It has recognized performance.
The relational person
The person is relational.
Human beings are formed, sustained, harmed, protected, and repaired through relationships.
Institutions, however, routinely isolate persons from the relations that constitute their lives.
The patient appears without the family that cares for them.
The student appears without the home and community shaping their learning.
The benefits applicant appears without the dependents whose survival is bound up with the claim.
To recognize only the isolated individual is to miss part of the person’s moral reality.
The person is irreducible, but not self-enclosed.
The narrating and credible person
The person narrates—and must be believed.
Persons do not merely present data. They give accounts of themselves.
Testimony, memory, pain, fear, identity, refusal, and self-understanding are part of how a person appears as a moral subject.
Institutions tend to transform narrative into fields, checkboxes, summaries, codes, and eligibility statements. The person’s account gets shortened, flattened, or mistranslated.
Even when a person speaks, they may not be believed.
Credibility is not distributed evenly. Some persons must do substantially more work to be believed because of race, disability, poverty, psychiatric history, carceral status, age, gender, sexuality, or the way they communicate.
Ethical recognition requires that the person’s account remain capable of correcting the record.
The situated and temporal person
The person is situated in history and changes over time.
Personhood is universal. Institutional vulnerability is not.
Race, gender, class, disability, sexuality, age, citizenship, poverty, illness, and carcerality shape how persons become visible or invisible within institutions.
The same category may protect one person, expose another, and erase a third.
Persons also change over time while records often do not.
A diagnosis, risk score, behavioral file, or credibility deficit may follow a person long after the reality it described has changed.
Ethical institutions must therefore practice re-recognition.
Records must remain provisional, revisable, and answerable to the living person.
The person’s claim to opacity
Finally, the person has a claim to opacity.
Recognition is not total visibility.
Institutions may need to know enough to care, protect, educate, support, or repair. But that need does not give the institution a moral claim on the whole person.
A person should not have to surrender their entire self in order to receive institutional response.
Ethical recognition must be proportionate: enough visibility to answer need, enough restraint to preserve dignity.
The person as the measure of the institution
The theory of the person establishes the moral foundation for everything that follows.
Institutions are accountable because they act upon persons.
Their forms, categories, scores, records, diagnoses, and procedures carry moral weight because they shape who can appear, what can be known, whose testimony can matter, and what response becomes possible.
A system that cannot recognize persons without reducing them is ethically defective, even if it is efficient, consistent, or technically accurate.
Across every institutional description, the person retains a moral excess that no category can exhaust.
The person is the measure of the institution.
The category must remain answerable to the person.
The record must remain subordinate to the life.
No person should have to become less human in order to be seen.
This is important as we see the evolving of individuals and pathology. Great read!