

A Polite Substitution Is Still a Substitution
On “intellectually challenged,” intellectual disability, and the lives institutions stop trying to know

Somewhere right now, a file describes a person as having an intellectual disability. That is the formal category. Or, in softer institutional language, the file calls them “intellectually challenged.” That is the euphemism, the gentler phrase, the term often chosen by people and institutions who believe the word itself has done the moral work.
The eligibility category says it. The care plan says it. And the institution that holds the file acts as if it now knows what it needs to know.
It does not.
The wrong is not inaccuracy
The wrong here is not that the category is inaccurate. It may be accurate in a narrow, administrative sense. The person may indeed have support needs, communication differences, or cognitive disabilities that require accommodation, assistance, or different forms of response. Naming those needs is not the problem.
Nor is this an argument against disability identity, disability pride, or the legal and political necessity of disability categories. Many people rightly claim “disabled” as a name for shared reality, access, solidarity, and rights. Institutions need categories to allocate support, authorize services, coordinate care, and protect rights.
The problem is not category. The problem is closure.
The problem is not category.
The problem is closure.
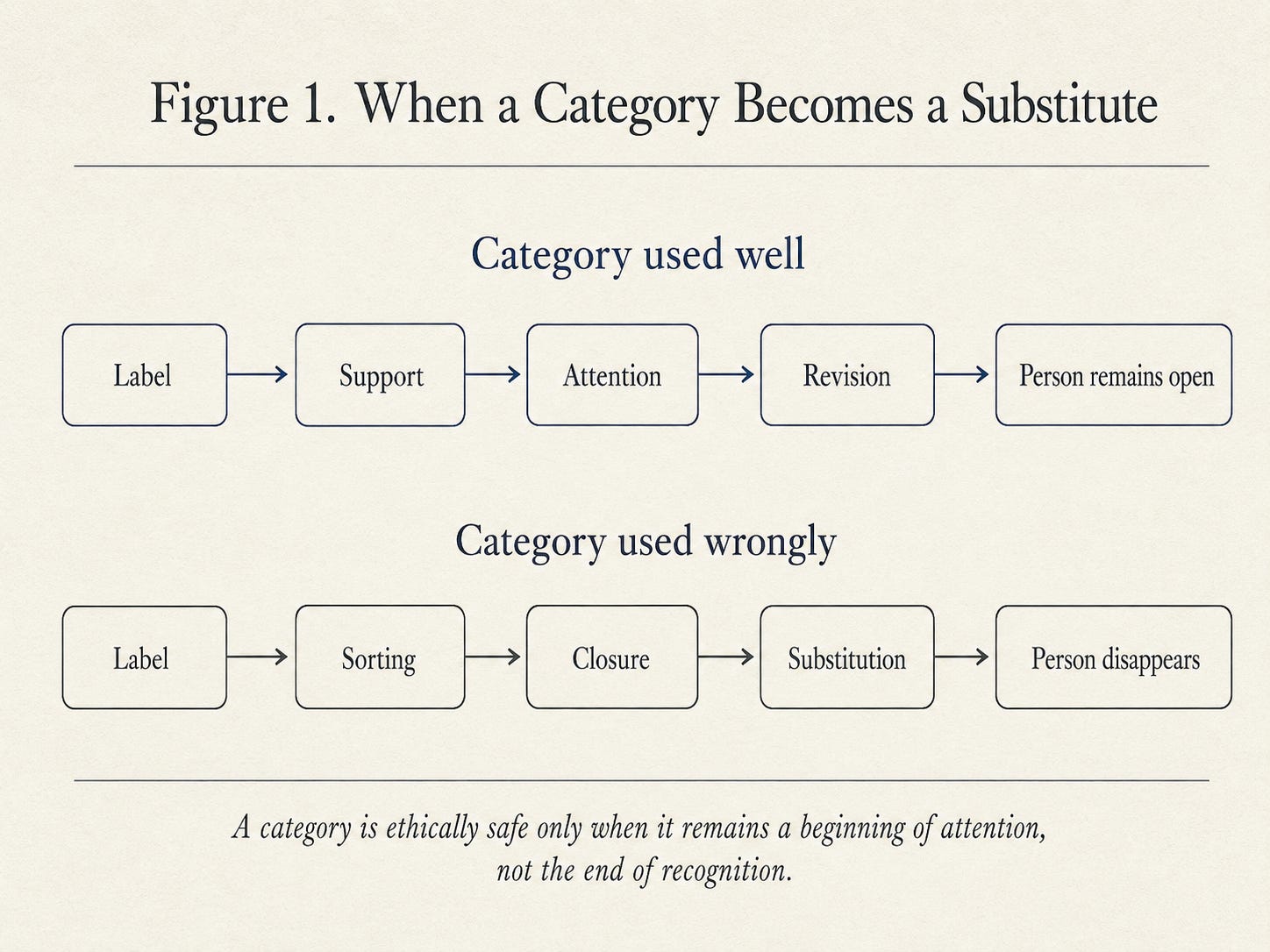
The target here is narrower: the institutional use of a category as terminal knowledge. The category may begin as a tool for response, but it becomes morally dangerous when it allows the institution to stop asking who this person is, what this person understands, how this person communicates, and what the institution itself may be failing to receive.
The wrong is substitution: the term is allowed to stand where the person should remain.
When an institution applies the label and stops there, the category claims jurisdiction over the person and then closes the case. But the institution does not know what the person experiences from the inside. It does not know what the person understands but cannot express. It does not know what the person’s inner life contains: memory, fear, love, grief, humor, longing, recognition, pattern, beauty. It does not know what forms of intelligence its own measures fail to capture.
This is not a demand that institutions treat every case as infinitely open. Institutions must make decisions. They must decide eligibility, placement, support level, risk, staffing, treatment, accommodation, and funding. The ethical demand is not paralysis. It is humility. The category may authorize action, but it must not become total knowledge. It may open a door, but it must not close the person inside the term.
The term becomes a substitute for the person. It belongs to the same family of wrongs as the slur, the risk score, and the diagnosis that becomes the patient. The tone differs. The mechanism is continuous. In each case, a word or form is permitted to do the moral work of attention.
The euphemism treadmill
The older terms—”imbecile,” “moron,” “feeble-minded,” “retarded”—are now recognized as slurs. It is worth remembering what they were before that. They were clinical categories. They were the polite terms. They were what institutions used to name and sort, and they were used by professionals who believed themselves respectful.
“Intellectual disability” is the current formal category. It can be necessary for services, law, education, and support. “Intellectually challenged” is different. It often functions as a softened substitute, a way of seeming kinder than the clinical term. That softening is not meaningless. Tone matters. But tone does not decide whether recognition has occurred.
A euphemism can still substitute. A formal diagnosis can still substitute. They do it in slightly different ways. The euphemism reassures the speaker that they have been gentle. The diagnostic category reassures the institution that it has been precise. But neither gentleness nor precision guarantees recognition.
“Intellectually challenged” is not automatically different in kind when it is used to close inquiry. It is different in tone: softer, more clinical, more careful. But when it allows the institution to name, sort, and stop looking, it performs the same structural work.
The politeness only makes the substitution harder to see. The institution says the gentler words and believes it has been respectful. But respect is not recognition. A polite substitution is still a substitution.
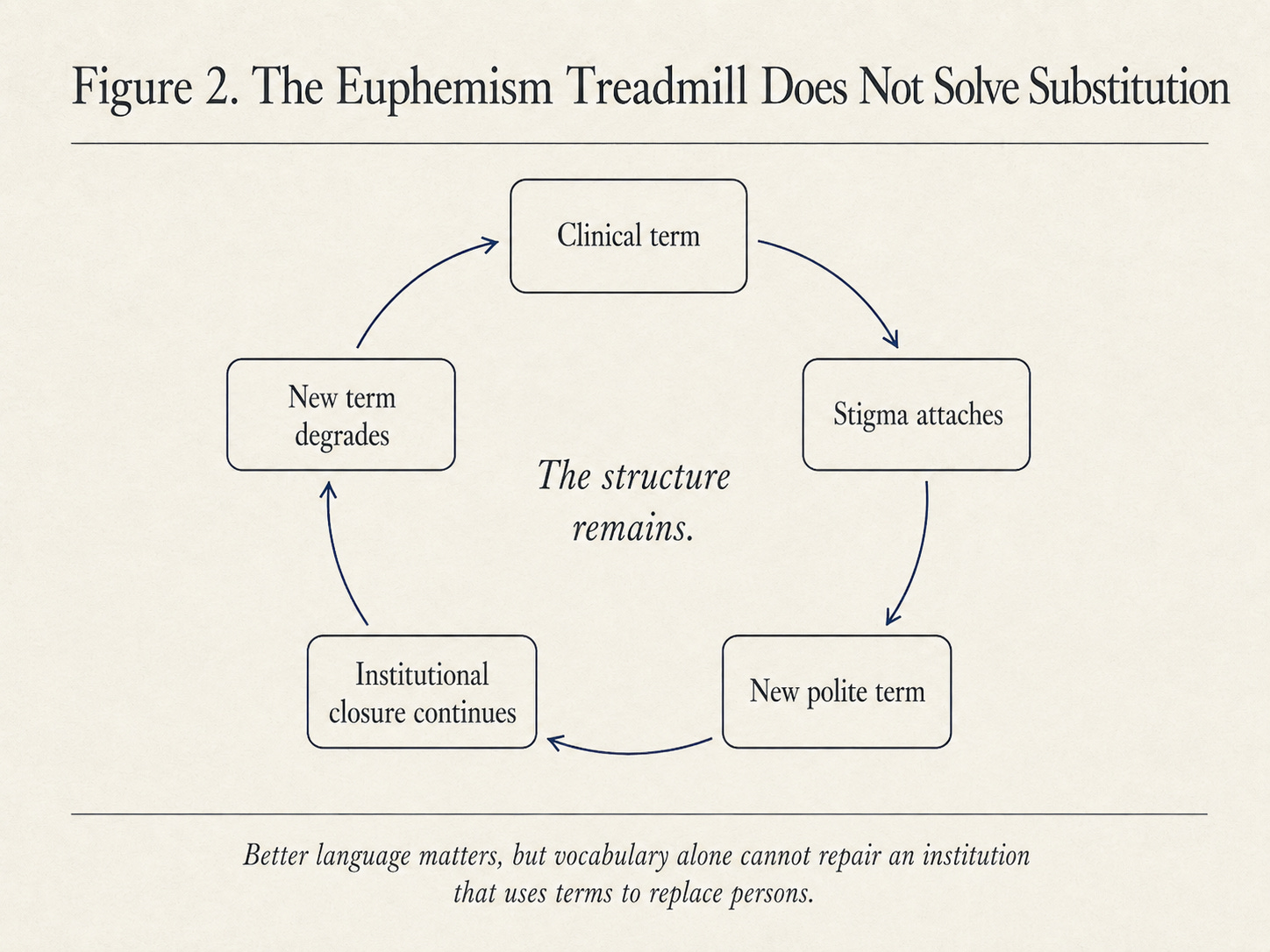
The arc of these terms is predictable. A clinical term becomes a slur. A new clinical term replaces it. The new term degrades in its turn. Linguists call this the euphemism treadmill, and the usual explanation is that the stigma of the condition contaminates each new word. I think that explanation is incomplete. The deeper reason is that the structure of substitution outlasts any particular word.
As long as an institution uses the term to replace the person rather than to reach the person, any term will eventually become degrading. You cannot solve a structural wrong with better vocabulary.
The denial of inner life
This is the deepest layer of the wrong.
The person the file describes has a life the file does not contain. That life may include love, grief, hope, fear, beauty, injustice, memory, anticipation, attachment, frustration, pleasure, humor, and meaning. There is no contradiction here. A limitation in expression is not a limitation in experience.
But the institution does not ask about that inner life. The category does not require it. The file has no field for it. The person may understand their situation perfectly, may know they are being reduced, may feel the condescension, may experience the substitution as a wound, and yet be unable to communicate that understanding in the institution’s preferred form.
The institution then mistakes inability to translate for absence of inner reality.
I know something of this from the inside. My own thinking is often vivid, organized, and immersive before it is verbal. Sometimes when I ask myself a question, the answer does not arrive first as a sentence. It arrives almost like a video: image, sound, pattern, feeling, memory, relation, meaning. When I am really thinking, speech can become difficult, not because nothing is happening, but because too much is happening in a form that does not immediately become words.
I do not offer this as a claim that my experience is identical to intellectual disability. It is not. I offer it as evidence of a simpler truth: outward verbal performance can radically understate inner life.
Let me be precise about what this argument is not. I am not claiming that we always know what is present in another person’s inner life. We do not. Some understanding may be partial, changing, inaccessible, or unlike anything the institution knows how to interpret. The ethical position is not sentimentality about hidden brilliance. It is agnosticism joined to dignity.
The institution does not know enough to presume absence, simplicity, or deficiency. And the person does not need to prove an impressive inner life in order to be owed recognition. Opacity is not permission for reduction. It is an invitation to humility.
Philosophers have a name for part of this: hermeneutical injustice. Miranda Fricker uses the term for the wrong that occurs when a person’s experience cannot become intelligible because the shared interpretive resources are missing. But the institutional version has a particular shape. Sometimes the problem is not only that the words are missing. It is that the form has already decided which words would count.
The person may be trying to communicate, but the institution has not built a place where that communication can arrive as knowledge. The form is not looking. The category has already told the institution what there is to know.
What the measures measure
Standard intelligence measures—IQ tests, cognitive assessments, academic performance, verbal fluency—capture a narrow band of human capacity. In many institutional settings, they privilege speed over depth, verbal expression over internal understanding, abstract reasoning over relational attunement, individual performance over collaborative sense-making, and familiar cultural frames over other ways of knowing.
What falls outside that band is not nothing.
Relational intelligence falls outside it: the capacity to read a room, recognize safety or danger, notice distress, respond to another person’s emotional state, and know who is present and who is only performing presence. The person who cannot answer a test question may still know who is kind. They may know who is rushed, who is irritated, who is pretending, who is trustworthy, who is afraid. They may understand the emotional weather of a room more accurately than the professional holding the clipboard.
The intelligence of care also falls outside it: anticipating need, holding attention, sensing rhythm, responding to another person’s state before that state has been formally named. A person may not be able to explain a moral situation abstractly and still know, in practice, when someone needs gentleness, distance, repetition, quiet, food, touch, or time.
Some assessments are more careful than this. The better ones consider adaptive behavior, communication context, community environment, cultural and linguistic difference, coexisting strengths, and support needs. The problem is not assessment as such. The problem is what happens when assessment becomes institutional permission to stop learning.
Imagine a form of intelligence that is embodied, relational, rhythmic, practical, and deeply attuned to others, but not easily translated into abstract verbal performance. Now imagine an institution that treats abstract verbal performance as the gateway to recognition. The failure is not simply in the person. It is in the institution’s decision to treat one narrow mode of expression as the measure of reality.
This is not hypothetical. Many people alive today—people with aphasia, with cognitive disabilities, with traumatic brain injury, with dementia, with forms of autism that affect verbal expression—are vulnerable to being misread in this way. Many understand more than the institution assumes. Many feel, recognize, remember, and know in ways the institution has not learned to receive. They cannot always translate what they know into the institution’s preferred form.
And even where understanding is partial, changing, or inaccessible to others, personhood is not reduced by the institution’s inability to measure it. That is not a retreat from the argument. It is the argument at its strongest. Dignity does not wait for proof of cognitive richness. The person is not less real because the institution cannot measure what is there.
The institution then treats the label as enough.
What recognition would require
I am not arguing for the abolition of categories. Institutions need categories to function, and people with disabilities need categories to access support. The argument is narrower and harder: the category must remain open. It must function as a beginning of attention, not the end of it. It must be held as partial, revisable, and answerable to the person it names.
A person-preserving institution would treat the category as a prompt for further attention. What does this person understand? How do they communicate? What supports make expression possible? Who knows them well? What does the category reveal, and what does it obscure? What capacities does the assessment fail to notice? What would allow this record to be revised if it has mistaken the category for the person? How can the record remain open to correction by the person, by those who know them, and by forms of knowledge the institution did not initially recognize?
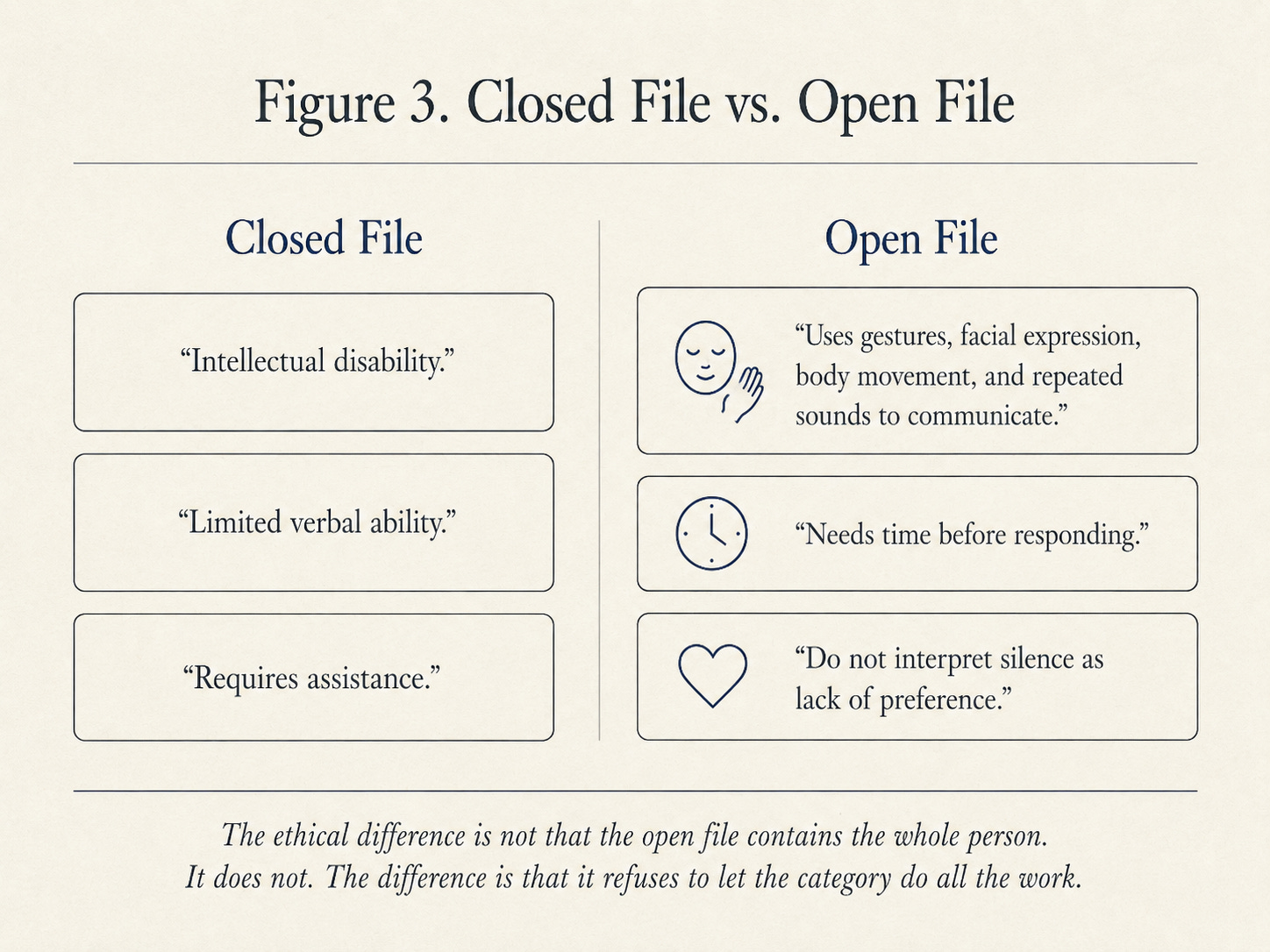
This does not have to remain abstract. A closed file says: “Intellectual disability. Limited verbal ability. Requires assistance.” That may be administratively useful, but it tells the institution almost nothing about how to meet the person.
An open file would say more. It might say: “Uses gestures, facial expression, body movement, and repeated sounds to communicate. Needs time before responding. Understands more when instructions are given slowly and paired with visual support. Becomes distressed when unfamiliar staff rush physical care. Recognizes familiar people and calms when addressed by name. Sister reports that humming means anxiety, not refusal. Reassess communication supports every three months. Do not interpret silence as lack of preference.”
That is still a file. It is still partial. It still does not contain the person. But it is morally different because it refuses to let the category do all the work. It treats the person as someone still to be learned from, not as someone already known.
I am not proposing a new form to fill out. Forms will always be forms. I am pointing to a posture that the form either permits or prevents.
The same is true of a care plan. A closed care plan says: “Nonverbal. Unable to participate in decision-making.” An open care plan asks: “How does this person show assent, refusal, discomfort, recognition, enjoyment, fatigue, fear, or trust? Who can help us interpret without speaking over them? What communication supports have been tried? What conditions make response more possible? What have we mistaken for noncompliance that may actually be distress, pain, overload, or distrust?”
Some practices already point in this direction: communication passports, serious assessment for augmentative and alternative communication, supported decision-making, circles of support, and rights-based approaches to communication. These practices do not solve the problem by themselves. They matter because they begin from a different institutional posture.
Not: prove someone is in there.
But: build the conditions under which this person can be received.
That shift matters. It changes the ethical burden. The person does not have to become fluent in the institution’s preferred form before they count as fully present. The institution has to become less confident that what it cannot receive is not there.
I recognize the institutional impulse to close the file because I have felt what it is to be filed.
The test of any term, polite or archaic, is the same: does the institution use it to reach the person, or to replace them? Every word we will ever invent for human difference will pass or fail on that question. The treadmill will keep turning until we stop asking which word is kind enough and start asking why the file is allowed to close.
The file has no field for the whole person. It never did. The ethical task is not to pretend that it can. The ethical task is to keep the file open to the life it cannot contain.
The person is still there, on the other side of the category.
They always were.